The article gives some additional detail regarding this attendee of a mostly peaceful literary event:
Hadi Matar, 24, was charged with attempted murder and assault and entered the plea during a proceeding at the Chautauqua County Courthouse…
He’s 24 years old and charged with attempted murder, according to the newspaper. Shouldn’t a potential SARS-CoV-2 infection be the least of his worries? (And isn’t that a proven-useless cloth mask, in any case?)
Science (as embodied in the CDC) now says that filthy deplorable germ-spreading unvaccinated people and clean virtuous vaccinated people should be treated the same with respect to coronapanic (see story from state-sponsored media below). Will Novak Djokovic then be allowed to play in the U.S. Open?
Separately, I am a little fuzzy on why anything should change for those who Follow the Science. According to the Google, COVID-19 killed 1,049 Americans on August 10, 2021. That level of carnage resulted in mask orders for public schools (but unmasked adults could spend an evening visiting the essential Marijuana shops of Massachusetts and then meeting new friends on Grindr or Tinder), forced vaccinations, the banishment of heretics from Twitter, Facebook, YouTube, etc. What was the level of carnage on August 10, 2022? 872 Americans killed. With a nearly identical number of deaths, for those who believe in the efficacy of mask orders, school closures, and forced vaccination, why give up these protective measures now?
The update isn't a huge overhaul of the existing guidance, but it does represent an increasing focus on individuals making their own decisions about their level of risk and how they want to mitigate that risk, said Dr. Marcus Plescia, chief medical officer for the @ASTHO. pic.twitter.com/GDEd1twhzi
One of the enduring mysteries of coronapanic is how the economy stayed so apparently healthy for so long. Unless gathering people together in an office was worthless, people working from home in 2020/2021 should not have been as productive as they had been in 2019. Unless education is worthless from an economic point of view, Americans in lockdown states who missed 1-2 years of education shouldn’t have been as productive as their counterparts in 2019.
U.S. labor productivity declined for the second consecutive quarter as overall economic output contracted and employers spent more on labor as they added workers.
U.S. nonfarm labor productivity—a measure of goods and services produced in the U.S. per hour worked—fell at a seasonally adjusted annual rate of 4.6% in the second quarter from the prior quarter, the Labor Department said Tuesday. Economists surveyed by The Wall Street Journal had estimated a drop of 5%.
On a per-hour basis, in other words, Americans generated less value.
Unit labor costs, a measure of worker compensation and productivity, increased at a 10.8% pace in the second quarter from the prior quarter, Labor said. Economists had expected a 9.5% increase.
“The trend in productivity growth has worsened compared to prior to the pandemic, and the surge in unit labor costs makes the Fed’s challenge of getting inflation back down to its 2% target all the more challenging,” Wells Fargo economist Sarah House said in a research note.
In other words, the cost of getting Americans off their sofas and into a productive situation, from an employer’s point of view, is higher.
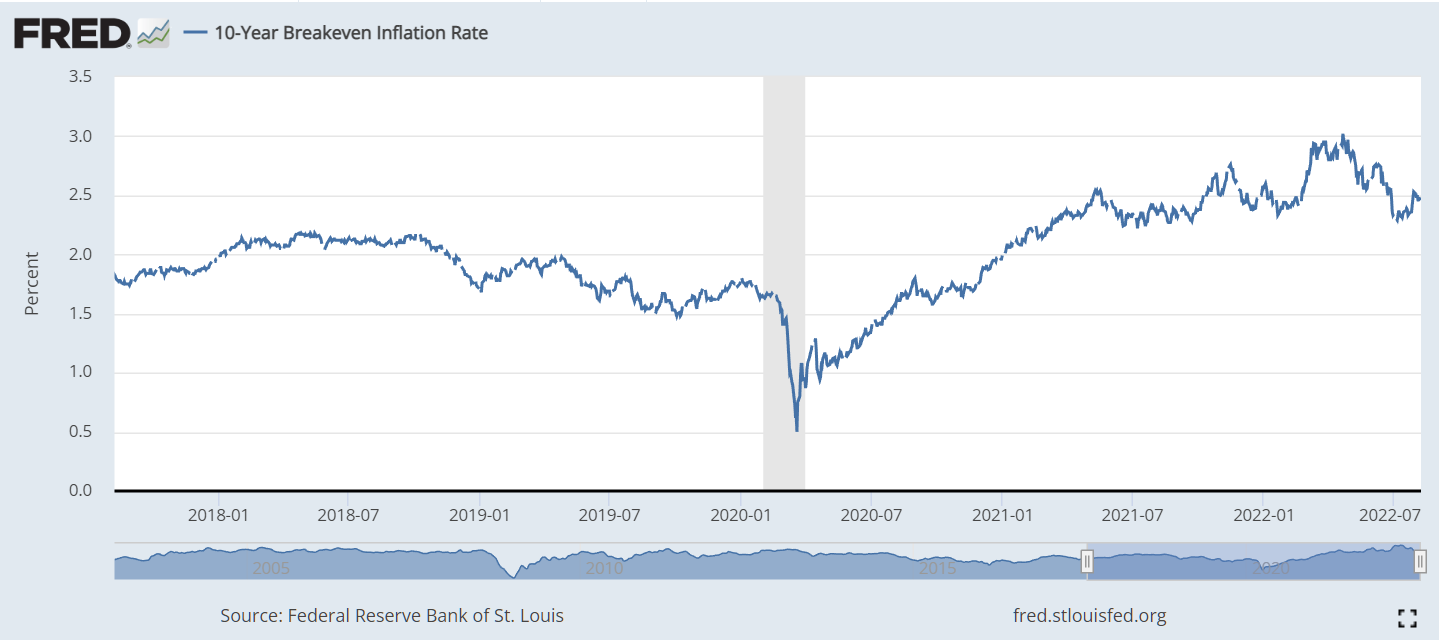
The only thing that I hate more than intolerance and hate is saying that markets are wrong, but I don’t understand how the bond market can be right in this case. If it costs companies more to produce everything, how do prices go up only 2.5 percent per year?
Despite being nearly 100 percent Deplorable-free (as commenter Angry Australian notes, the handful of “rightwing nutjobs” who did not appreciate the healing powers of essential marijuana, lockdown orders, forced masking, and vaccination papers checks have likely moved away from the State of Science into the famously Republican strongholds of Miami Beach and Palm Beach County), Massachusetts is apparently rejecting the Sacrament of Fauci for its most vulnerable residents. “11% of Children Under 5 Have Received COVID-19 Vaccine in Mass.” (NECN, today):
Before COVID-19 vaccines were rolled out for children under the age of 5 back in June, many parents had been calling for those shots to become available for young kids.
But new data looks like some parents’ stance may have changed.
Massachusetts ranks third nationwide, with 11% of those kids getting at least one dose, according to The Boston Globe. Washington D.C. took the top spot, with nearly 18% and Vermont came in at second place.
Pediatricians say they did expect some hesitancy, and according to the Globe, surveys predicted that only around one in five parents would actually plan on getting children in that age bracket vaccinated. The numbers so far are lower, though, than many pediatricians expected by this point. The vaccination rates for these young children are lower than any other age group in the state.
As a result, some doctors say they’ve actually had to throw some of these vaccines out because they’re not being used.
How can this be? The COVID-19 vaccine for young children was Emergency Use Authorized by the FDA. Therefore, young children are facing a health emergency. Yet the smartest people in the United States are not Following the Science and applying proven-by-Science emergency remedies to ameliorate the emergency.
Loosely related, I found Dr. Fauci’s most recent book for kids at a toy store in Amana, Iowa:
U.S. Open organisers also said that while they do not have a vaccination mandate in place for players, they will respect the U.S. government’s position regarding travel into the country for unvaccinated non-U.S. citizens.
Another post with the same hashtag brought up U.S. President Joe Biden, who is fully vaccinated and twice boosted but tested positive on Saturday just three days after having emerged from isolation after testing positive for the first time on July 21.
“Quadruple-vaxxed Biden tested positive for Covid again. But unvaccinated Covid-recovered Djokovic can’t play in U.S. Open. He is apparently too big a risk to the U.S. healthcare system,” the tweet read.
Monkeypox is a global health emergency. But bathhouses are “essential” from a public health point of view and won’t be shut down despite the potential for monkeypox to thrive in our bathhouses.
Combining the above, could Novak Djokovic be admitted to the U.S. if he says that his reason for travel is to visit a bathhouse?
Any successful response to an outbreak needs to be grounded in facts, and the facts are clear. Out of the cases recently reported to the W.H.O., data on sex is available for about three-quarters. Of these, about 99 percent are male. Data on sexual orientation is available for only about 7,500 cases, but of these, 97.5 percent are men who have sex with men.
A two-page leaflet by German health authorities to inform the public about monkeypox does make clear that spread is happening in places like sex clubs. But it does not mention the words “gay” or “men who have sex with men” once.
Even within my own community, some have argued that stating that the disease was mostly affecting men who have sex with men was homophobic. Others were simply afraid of worsening the stigma many gay men already face. On the other end of the spectrum, social media accounts that have gained huge numbers of followers during the coronavirus pandemic are spreading the false information that monkeypox is transmitting widely through handshakes, the food we eat and the air we breathe. The result has been confusion, with some people wrongly thinking they are at high risk and others not knowing about their very real risk or how to lower it.
(When will Los Angeles, San Francisco, Chicago, Boston, and New York City close the public schools to protect children from this disease?)
From the Amana Colonies, the passionate Christianity of the 19th and 20th centuries is now passion for 2SLGBTQQIA+ love plus commonsense gun safety laws:
According to a new report by the CDC, one in five COVID survivors under the age of 65 has experienced a health condition that could be considered long COVID. For seniors, that number rises to one in four.
So… the typical older American has a 25 percent chance of experiencing Long COVID while Joe Biden’s chance is 0 percent. Our leader will not suffer from brain fog.
A friend with a Ph.D., on hearing the news about Joe Biden’s COVID-19 situation:
Does he have Covid, cancer, dyslexia, dementia, or more? I have no idea.
Meanwhile, we visited Dollywood this week (en route to Oshkosh via Cirrus SR20). The crowds were manageable (much more so than in Great Smoky Mountains National Park, which has 1/5th of the infrastructure that it needs to handle the volume of visitors), but it was still a crowded environment. We saw a family wearing masks. Father in a surgical mask. Son in a cloth mask. Mom wearing a chin diaper. They were concerned enough about COVID-19 to wear masks, but not concerned enough to refrain from visiting a jammed theme park. My personal solution for keeping safe from COVID-19 is to avoid obesity via consuming all-natural pork rinds. Here is the Dollywood pork rind operation:
(In fairness, the rate of obesity at Dollywood seems to be lower than at Disney World.)
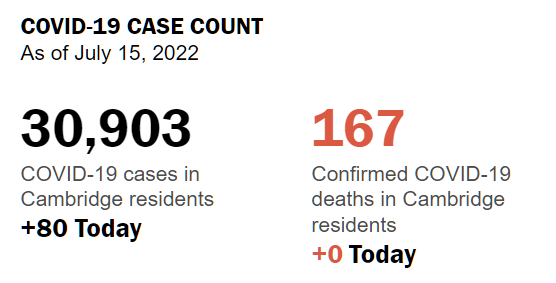
I’m still on the mailing list for City of Cambridge (Maskachusetts) updates. Every day they send out their dead pool data. From yesterday:
Nobody died yesterday in Cambridge because everyone got the Sacrament of Fauci, right? The Harvard-educated Democrat-voting folks in Cambridge wouldn’t contribute to coronaplague by running around unvaccinated like the Deplorables in the Unspeakable Republican South, certainly. Well…
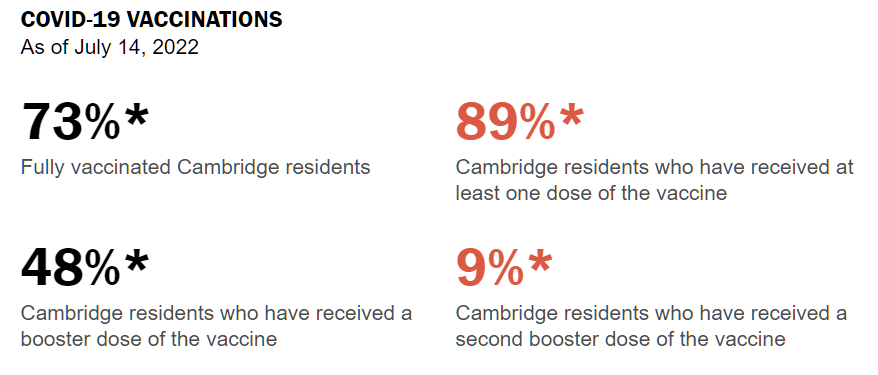
Only 73 percent fully vaccinated?!!? Now that vaccines are emergency-used authorized for 6-month-old babies, how can this be? And how does this compare to a state in which public health authorities do not promote the idea of injecting children with experimental medicines that are designed to prevent deaths among the elderly? The percentage of Floridians (DeSantis voters!) who are fully vaccinated is currently 68 percent. Maybe the answer for how the intelligent people who live next to MIT and Harvard can have such similar vaccination coverage to the morons of Florida is that the newly approved COVID shots for babies require at least 8 weeks for the baby to be considered “fully vaccinated” and the emergency use authorization for sticking babies was issued only a month ago.
A young relative was pleased to find that bars in the U Street area of Washington, D.C. are vigilantly checking vaccine papers despite the fact that the government’s order for bars to check has expired. “I had to show photo ID and my vaccine card, which they checked carefully,” he explained, “but they run out of energy before they get to the birthdate field so I was able to get in and order whatever I wanted.”
(He’s fully vaccinated not because of #FaithInFauci, but because he was forced to get stuck with an experimental medicine, designed to prevent death among people who are 60 years older than he is, as a condition of continued enrollment at a university.)
When coronapanic began, the CDC told Americans that, contrary to all previously established medical knowledge, a simple cloth or surgical mask would substantially prevent infection by SARS-CoV-2. This advice has been walked back, to some extent, in favor of suggesting N95 masks, but the general public does not seem to have gotten the more recent memo.
On a June trip to San Diego, I noticed a fair number of people who apparently sought to protect themselves and others from COVID-19. Instead of staying home, which would have been the obvious choice given pre-2020 Science, they were on 100-percent-crammed airline flights, in museums, etc.
Here is an example from the Chick-fil-A line in Atlanta:
An example on the deck of the USS Midwayin San Diego (awesome museum, but staying home is safer):
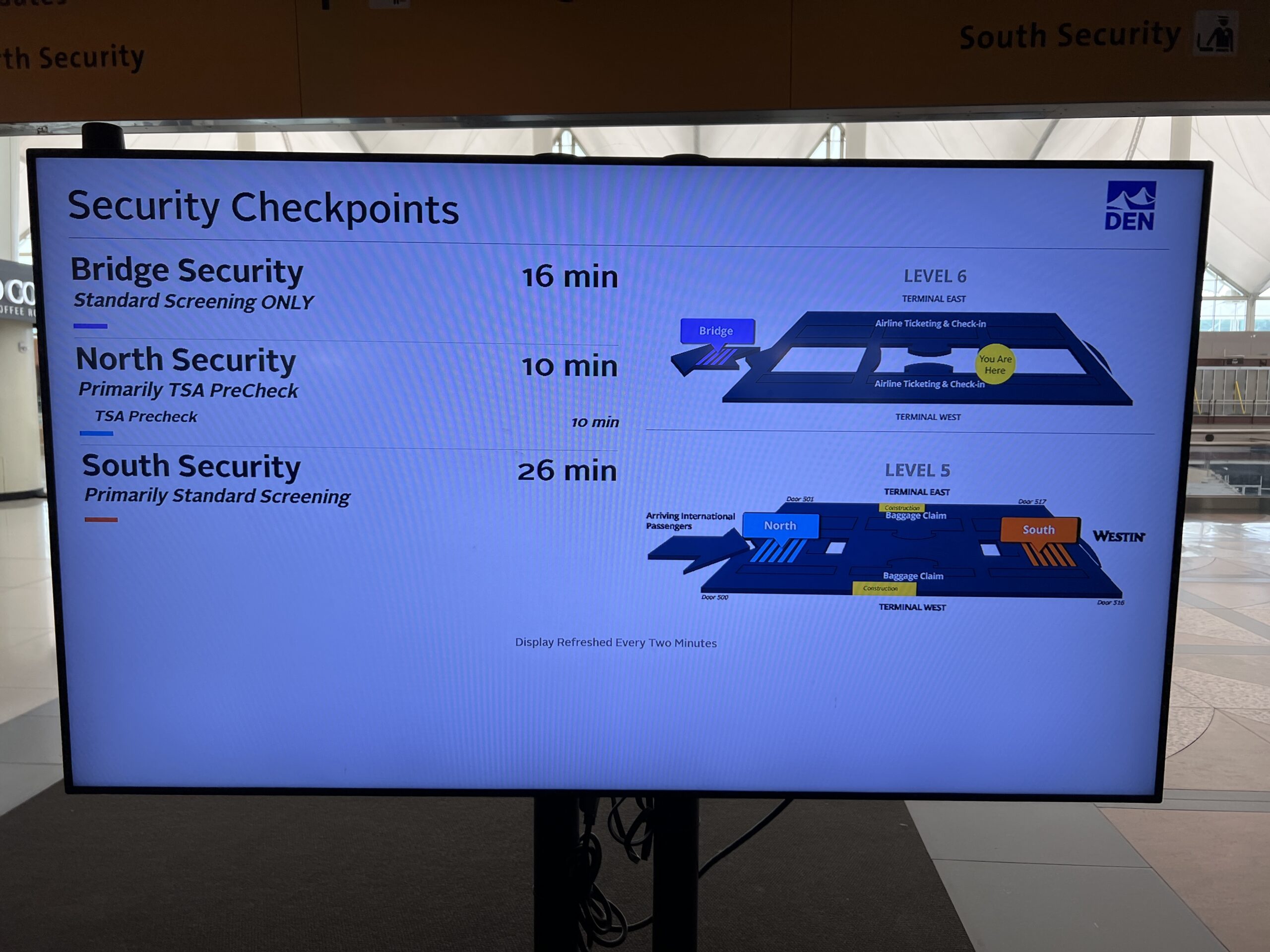
Despite half of the U.S. taking the position that avoiding COVID-19 is a critical human activity and that the other half of the nation is morally deficient for not sharing their concern, the Denver airport was crammed to capacity on a Wednesday at noon (imagine Friday afternoon before a holiday weekend!). A 26-minute wait for the non-elite:
Colorado supported Joe Biden, but it seems that the typical local won’t wear a mask while engaging in a religious ritual at the Denver airport’s 2SLGBTQQIA+ monolith (imagine the joy if Kubrick’s 2001 were updated with this monolith!):
On a related note, the Delta flight attendant offered me an alcohol wipe during boarding. I replied, “thank you, but my personal hygiene problems are far too severe to be addressed by one wipe.”
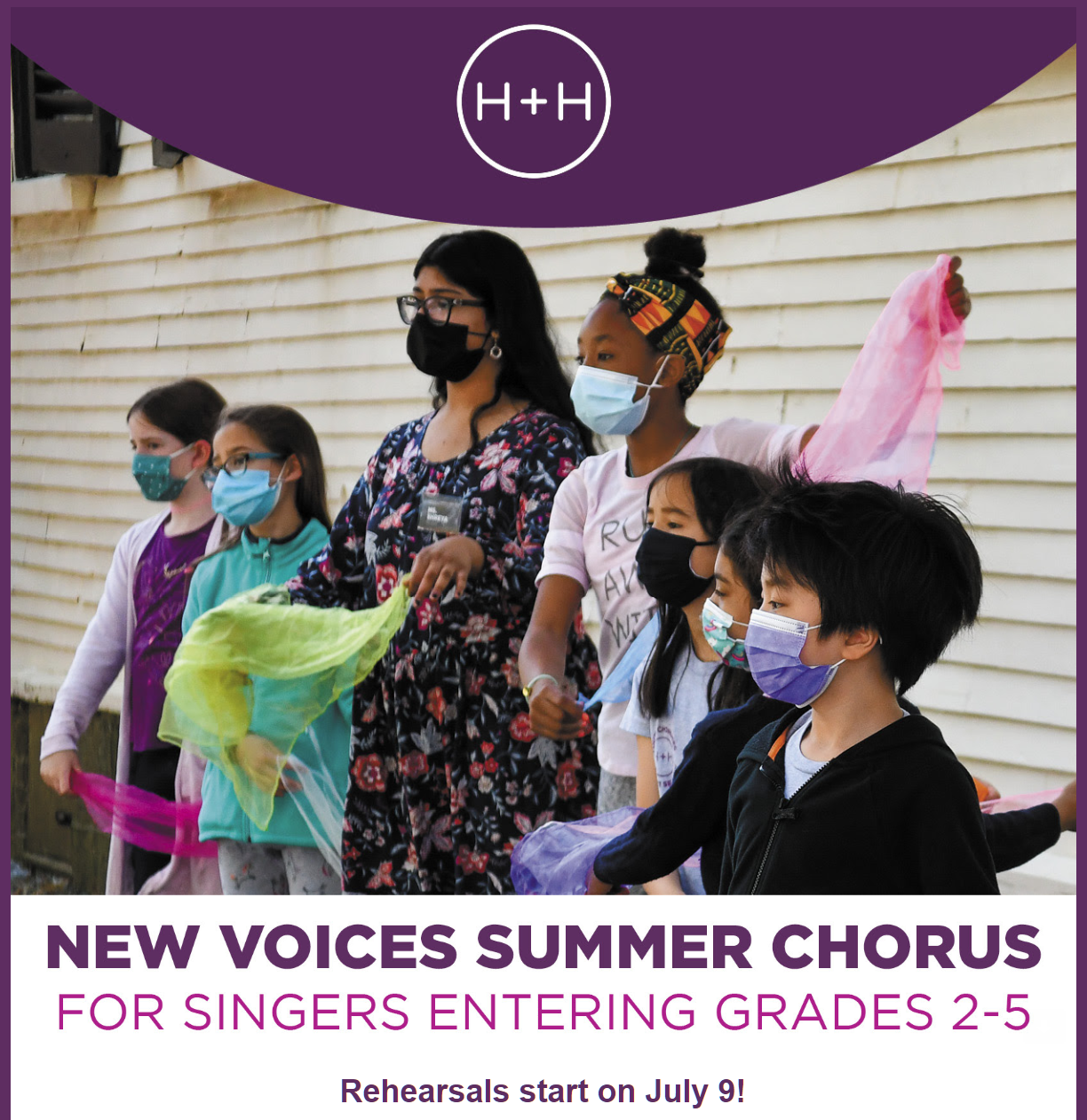
All participants in H+H Youth Choruses activities must be fully vaccinated for Covid-19, and we provide further that H+H agrees to comply with the then-applicable U.S. Equal Employment Opportunity Commission (EEOC) guidance regarding mandatory employer vaccination programs. Masks are required for all indoor activities at all times.
Recall that, like California, Massachusetts is a state that decided marijuana shops for adults were “essential” and had to remain open while public schools were closed for 1.5 years and forcibly masked for at least 1 additional school year (unclear what will happen in the Boston Public Schools for 2022-2023).