Relocation to Florida for a family with school-age children
TL;DR: We decided that the west coast was too old, that Miami was too congested, and that Jupiter, Florida, specifically the MacArthur Foundation-planned Abacoa section, was perfect.
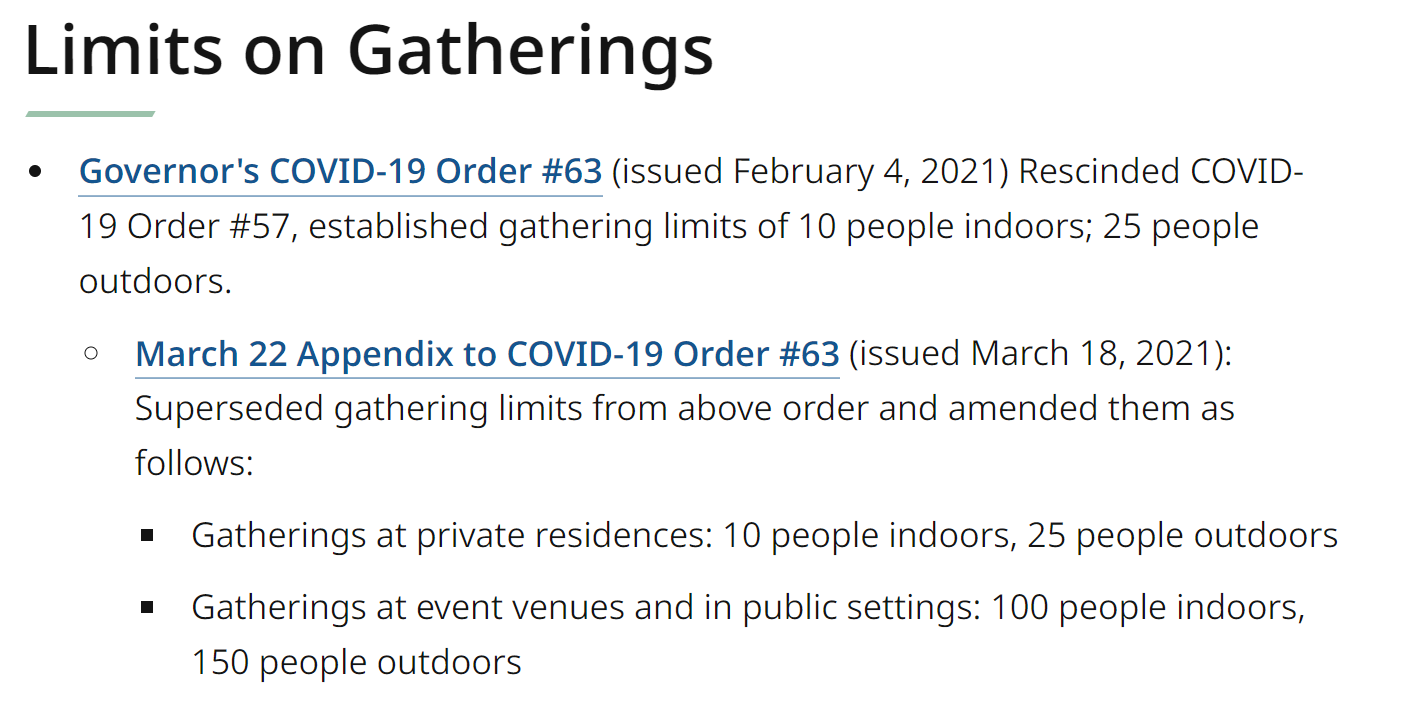
Prior to 2020 the political control of a state or town had little impact on day-to-day life, with the exception of custody, alimony, and child support law. Republicans and Democrats might disagree regarding tax rates, government spending, zoning regulations, etc., but not about whether it should be legal to leave one’s house, go to work, attend school, breathe without a mask, interact with other humans without getting an injection, etc. After 2020, however, it is unclear why anyone would choose to be part of a political minority. For a Democrat, being in a Republican-run state means risking death from respiratory viruses that aren’t being controlled with Science (lockdowns, mask orders, coerced vaccination, 12-18-month school closure). For a Republican, being in a Democrat-run state means that one’s children aren’t guaranteed an education (though they might get surgery and show up at the breakfast table sporting a different gender), that one might lose what had been First Amendment rights, e.g., freedom of assembly, and that one will be surrounded by virtuous yard signs and bumper stickers.
For a Republican escaping a Democrat-run state, it doesn’t make sense to move to a place with a state income or estate tax (see Effect on children’s wealth when parents move to Florida). So the search process starts with intersecting the states that remained relatively free during coronapanic and income-tax-free states, which yields South Dakota, Alaska, Florida, and Tennessee. South Dakota is an awesome state for domestic asset protection trusts (along with Nevada, this is where America’s billionaires keep their trusts, but the ultimate protection may not work unless you live in SD or NV) and thus is a good place to preserve wealth from potential plaintiffs. It is a lovely place to spend the summer, but if you have school-age children you might not enjoy being stuck there December through February. With apologies to friends in Anchorage, that goes double for Alaska! Now we’re down to Florida and Tennessee. Nashville, for example, is reasonably nice in January, with average highs of 48 degrees, but Tennessee is more of a working state than a fun/retirement state. If you’re going to move, why not move to a playground? And Miami, oddly enough, despite being much warmer in winter is actually slightly cooler in the summer than Nashville. The WalletHub ranking of Coronafreedom may not give the full picture for Tennessee, whose governor declined the Central Tyrant job and did not order everyone to wear masks. However, unlike in Florida, where the governor forbade local tyrants from imposing mask laws with fines, the Tennessee governor simply delegated tyranny to counties: “Since the beginning of the COVID-19 pandemic, there has not been a statewide mask mandate in place in the state of Tennessee, however, local authorities were given the authority to issue mask mandates within their own jurisdictions.” A state with empowered local tyrants is not exactly free! Thus, as so many fleeing Wall Streeters have discovered, it all comes down to Florida.
This is a report on my own January/February exploration trip to Florida in the Cirrus SR20...
Gainesville. Beautiful campus for University of Florida, but not a beautiful or vibrant town. Apparently when the smart young people graduate they go somewhere else. Particularly unsuitable for aviation enthusiasts as the (great) airport is on the opposite side of town from the nicer real estate (tucked away in suburban developments that have a minimal relationship to Gainesville). At least with respect to Covid-19, the students seem smarter than the (cowering out of personal fear) Ivy League to whom I’ve talked recently. “We’d behave differently,” one sophomore said, “if we lived with our grandparents, but we don’t. There is no reason for us to be afraid of getting the virus and we live more than 100 miles away from our older relatives. Classes are mostly remote, so the only people that we interact with are other young people who aren’t at risk.”
Guess which department has the ugliest building? Note the students hunting for shark’s teeth in a nearby park and the selfie park at the FBO.







Sarasota. Folks with kids will want to live on the mainland rather than one of the islands (great for beach access, but the traffic can be slow getting on/off for the various services and activities that kids need). The neighborhood around the Southside Elementary School is probably the most desirable, with Camino Real being the best street and anything east of the Tamiami Trail being cheaper. Overall, however, Sarasota is more geared around the retired than those of school age. Great airport shared by air carriers and general aviation, about 13 minutes from the Southside school.
The Ringling (world’s only fine art and circus museum!) and the latest condo development for oligarchs (from my friend’s boat).



View from my friend’s apartment and his neighborhood from the air on departure…


Naples. A nice walkable downtown area. Attractive architecture. World-class restaurants at Manhattan prices (if restaurants in Manhattan were open!). There are some young people in town, but they’re apparently mostly tourists. As with Sarasota, dominated by the retired. In fact, the saying goes that “People retire to Sarasota so that they can visit their parents in Naples.” Great airport, 10 minutes from downtown, that is used only for general aviation. It was so busy in late January that jets parked on the ramp were interlaced like jets in a hangar (i.e., it wouldn’t have been possible to get one out of the middle without an hour or two of tugging).

Miami. The ultimate party town now that Los Angeles and New York have locked themselves out of the running and probably even before. “I can never get any work done here,” said one of the private equity guys I was with. KTMB is the preferred airport and it is a long haul from Miami Beach (nearly 40 minutes without traffic). KOPF is a little closer, but nobody seems to like it. If you aren’t going to hit the clubs and don’t have to be in the city for work, why put up with the congestion, traffic, and high real estate prices?
The Wynwood Walls (decluttered now that they’re charging $10 to get in), breakfast cereals for the Age of Coronapanic (Franken Fat, Cap’n Corn Starch, Obesie Os from Killkidds), transportation on which it would be good to get Dr. Fauci’s opinion regarding safety, and a group of #ScienceDeniers gathering at a rooftop club.




On the way out of town, the illegal-to-operate cruise ship pier:

Key West. We went there in a Cirrus Vision Jet to visit a Massachusetts friend who is passionate about kiteboarding and expanding government so that wise Democrats can accomplish more. As it happens, however, he lives in Key West 183 days per year and thus escapes Massachusetts state income and estate taxes. It will be folks other than him who pay for the bigger government that he advocates. Key West is so small that I think it would be tough to find specialized teachers, coaches, doctors, etc. for the modern-day helicopter parented child. The airport has a short-ish runway (5,000′) and is monopolized, with associated monopoly rates, by Bill Gates’s Signature Flight Support (jet fuel for private jet owners who are as concerned as Bill G about climate change).
Fun fact: Pan American World Airways began here. Cuba started out 90 miles away, but it is getting a little closer in spirit with every $1.9 trillion government spending bill… Found the Icon A5 on the ramp at KTMB (my flight in the A5 at Oshkosh).





Wellington Aero Club. West of Palm Beach, right up against the $25 million horse barns of America’s billionaires, you can open your garage door and taxi your twin-engine turbojet out to the 4,000′ private runway (FD38). Good public schools. Great country club for golf and tennis next door. I had a nice time here visiting a friend whose wife is a serious horse rider, but I wouldn’t want to be this far from the beach (30-40 minutes, depending on the specific beach). (See “How a Sleepy Florida Town Became the Horse Riding Capital of the World” and the 30-horse single-family stable below) My friend in Wellington (also a passionate advocate of bigger government who is careful to spend 183 days in the tax-free Land of the Deplorables!) suggested Abacoa, within Jupiter, Florida, as the best family location.





Jupiter: Palm Beach-Fort Lauderdale-Miami can be thought of as a single city, completely jammed, and with the automobile as the primary means of transportation. Juno Beach and Jupiter are the first communities on the north side of this megacity (though the Census Bureau considers them still part of the Miami metro area). The smartest folks in Germany, i.e., those who run the Max Planck Institute, picked Jupiter as the location for their one and only U.S. research lab (in neuroscience). If you’re in Jupiter you’re within a 1.5-hour drive of almost anything that you might need, e.g., the Miami International Airport and a nonstop flight to Europe, but 99 percent of needs can be handled locally. (Disney World is 2:20 away by car.) A tennis coach at the Jupiter Ocean & Racquet Club, a world class facility for (unmasked!) young learners and also great for adults, echoed my friend in Wellington regarding Abacoa, a MacArthur Foundation-created New Urbanism planned-but-not-gated community. “The schools for Abacoa are better than for the wealthier/closer-to-the-beach areas of Jupiter,” he said. [We later learned that the neighborhoods near the beach tend to be older and seasonal; not good for kids looking to play after school.] He pointed out that many of the nation’s most successful people, who could live anywhere they chose, had chosen to live in and around Jupiter. In a state that is blessed with magnificent airports, Abacoa/Jupiter got the short end of the stick. Palm Beach International is about 20 minutes away and the prices are almost reasonable due to the fact that there are three FBOs on the field. On the other hand, nobody is ever going to build T-hangars at KPBI. The North Palm Beach airport, F45, is roughly the same driving distance and it does have T-hangars, but the runway is a little short (4,300′), there is no control tower, and it is a monopoly Signature location (Jet A at $7.21/gallon; compare to $3.70 at Fort Lauderdale Executive (KFXE))
If you didn’t think inequality was as bad as the media tells you… (on the ramp at KPBI; 1960 Debonair and a newly certified Gulfstream G600):

Just south of the airport…


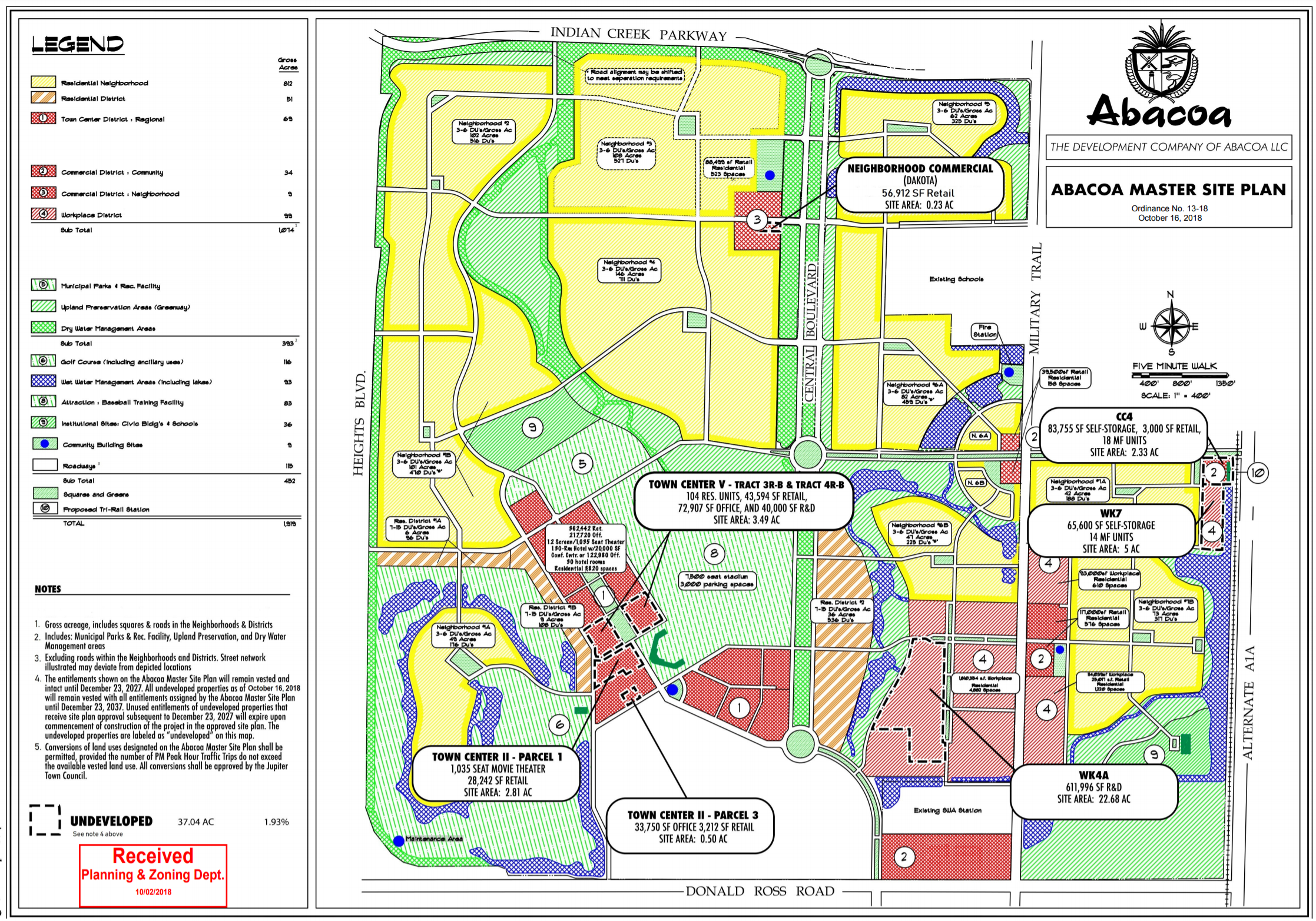
Abacoa. This is a planned “new urbanism” community, a bit like what you might have seen in the Truman Show movie (Seaside, Florida). It is an artificial town in that it is possible to walk/bike to a “town center”, which does have some good restaurants and a coffee shop, but the critical services, such as supermarket and Home Depot, are in strip malls on the edges or across a major road from Abacoa itself. Without traffic, it is an 11-minute drive to a beautiful dog-friendly beach.
That’s what I was able to learn in a two-week trip (including flying the Cirrus up and down the East Coast, which takes about 13 days, depending on the weather…). Measured by whether it is legal to walk out your door without a mask on, go to work, open the doors of your business to customers, send your children to school, let you children enjoy an unmasked after-school activity, etc., every part of Florida offers more freedom than New York, Massachusetts, or California. For someone accustomed to the suburban Northeast, the small yards and tightly packed houses seem like the biggest negative. In the parts of
Full post, including comments